Utilizamos cookies para habilitar las funciones necesarias para este sitio web, como el inicio de sesión o la cesta de la compra. Puede encontrar más información en nuestra política de privacidad.
Giulio Rasperini, DDS, is an associate professor of dentistry and periodontology in the Department of Biomedical, Surgical, and Dental Sciences at the University of Milan in Italy and an adjunct clinical associate professor in the Department of Periodontics and Oral Medicine in the School of Dentistry at the University of Michigan. He serves on the editorial board for The International Journal of Periodontics & Restorative Dentistry, has published and lectured extensively on periodontology and implantology, and is the recipient of several research awards. In 2017, Dr Rasperini founded the iPerio Education Center in Piacenza, Italy, with Dr Giorgio Pagni and Dr Raffaele Acunzo.
The 15th International Symposium on Periodontics and Restorative Dentistry (ISPRD)
junio 12, 2025 — junio 15, 2025Boston Marriott Copley Place, Boston, MA, Estados Unidos de América
Ponentes: Edward P. Allen, Evanthia Anadioti, Gustavo Avila-Ortiz, Christopher Barwacz, Florian Beuer, Nitzan Bichacho, Francesco Cairo, Vivianne Chappuis, Chia-Yu (Jennifer) Chen, Stephen J. Chu, Florin Cofar, Daniel Coleman, Luca Cordaro, Daniel Cullum, Luca De Stavola, Carlo Ercoli, Vincent Fehmer, Iñaki Gamborena, Maria L. Geisinger, William Giannobile, Luca Gobbato, Oscar Gonzalez-Martin, Jim Janakievski, Y. Natalie Jeong , Ronald Jung, Joseph Kan, Jihyon Kim, Gregg Kinzer, Christopher Köttgen, Ina Köttgen, Stefen Koubi, Purnima S. Kumar, France Lambert, Alejandro Lanis, Ernesto A. Lee, Paul Levi Jr, Tomas Linkevičius, Pascal Magne, Pamela Maragliano-Muniz, Konrad H. Meyenberg, Craig M. Misch, Ricardo Mitrani, Rodrigo Neiva, Giorgio Pagni, Gianluca Paniz, Giulio Rasperini, Pooyan Refahi, Andrea Ricci, Marisa Roncati, Paul S. Rosen, Irena Sailer, Mariano Sanz, Ignacio Sanz Martín, Ignacio Sanz Sànchez, Todd Scheyer, Frank Schwarz, Massimo Simion, Frank Spear, Martina Stefanini, Clint Stevens, Lorenzo Tavelli, Tiziano Testori, Sejal Thacker, Teppei Tsukiyama, Istvan Urban, Eric Van Dooren, Diego Velasquez, Hom-Lay Wang, Giovanni Zucchelli, Otto Zuhr
Quintessence Publishing Co., Inc. USA
4th Urban Regeneration Symposium
Timelessness in Regenerationoctubre 18, 2024 — octubre 19, 2024Vigadó Concert Hall (Pesti Vigadó), Budapest, Hungría
Ponentes: Edward P. Allen, Matteo Chiapasco, Lisa J. A. Heitz-Mayfield, Giulio Rasperini, Massimo Simion, Istvan Urban, Hom-Lay Wang, Giovanni Zucchelli
Urban Regeneration Institute
The 5th Smart Casual Dentistry Σymposium & XXII SE.NA.ME. International Conference
octubre 10, 2024 — octubre 12, 2024Athens Conservatoire, Athen, Grecia
Ponentes: Christos Angelopoulos, Rafael Beolchi, Nitzan Bichacho, Pietro Felice, Sotiria Gizani, Galip Gürel, Kostas Karagiannopoulos, Panagiotis Lampropoulos, Giulio Rasperini, Michele Temperani, Eric Van Dooren, Ioannis Vergoullis
OMNIPRESS
Rasperini Reunion International
junio 20, 2024 — junio 22, 2024Piacenza, Italia
Ponentes: Egon Euwe, Jaime Jiménez Garcia, Giulio Rasperini, Vincent Ronco, Monaldo Saracinelli, Anton Sculean
iPerio EDUCATION
The 14th International Symposium on Periodontics and Restorative Dentistry (ISPRD)
junio 9, 2022 — junio 12, 2022Boston Marriott Copley Place, Boston, MA, Estados Unidos de América
Ponentes: Tara Aghaloo, Edward P. Allen, Evanthia Anadioti, Wael Att, Vinay Bhide, Markus B. Blatz, Scotty Bolding, Lorenzo Breschi, Jeff Brucia, Daniel Buser, Luigi Canullo, Daniele Cardaropoli, Stephen J. Chu, Donald Clem, Christian Coachman, Lyndon F. Cooper, Daniel Cullum, Lee Culp, José Carlos Martins da Rosa, Sergio de Paoli, Marco Degidi, Nicholas Dello Russo, Serge Dibart, Joseph P. Fiorellini, Mauro Fradeani, Stuart J. Froum, David Garber, Maria L. Geisinger, William Giannobile, Luca Gobbato, Ueli Grunder, Galip Gürel, Chad Gwaltney, Christoph Hämmerle, Robert A. Horowitz, Marc Hürzeler, David Kim, Gregg Kinzer, Christopher Köttgen, Ina Köttgen, Purnima S. Kumar, Burton Langer, Lydia Legg, Pascal Magne, Kenneth A. Malament, Jay Malmquist, George Mandelaris, Pamela K. McClain, Michael K. McGuire, Mauro Merli, Konrad H. Meyenberg, Craig M. Misch, Julie A. Mitchell, Marc L. Nevins, Myron Nevins, Michael G. Newman, Miguel A. Ortiz, Jacinthe M. Paquette, Stefano Parma-Benfenati, Michael A. Pikos, Giulio Rasperini, Pamela S. Ray, Christopher R. Richardson, Isabella Rocchietta, Marisa Roncati, Marco Ronda, Paul S. Rosen, Maria Emanuel Ryan, Irena Sailer, Maurice Salama, David M. Sarver, Takeshi Sasaki, Todd Scheyer, Massimo Simion, Michael Sonick, Sergio Spinato, Dennis P. Tarnow, Lorenzo Tavelli, Douglas A. Terry, Tiziano Testori, Carlo Tinti, Istvan Urban, Hom-Lay Wang, Robert Winter, Giovanni Zucchelli
Quintessence Publishing Co., Inc. USA
Artículos de este autor en revistas
International Journal of Periodontics & Restorative Dentistry, Pre-Print
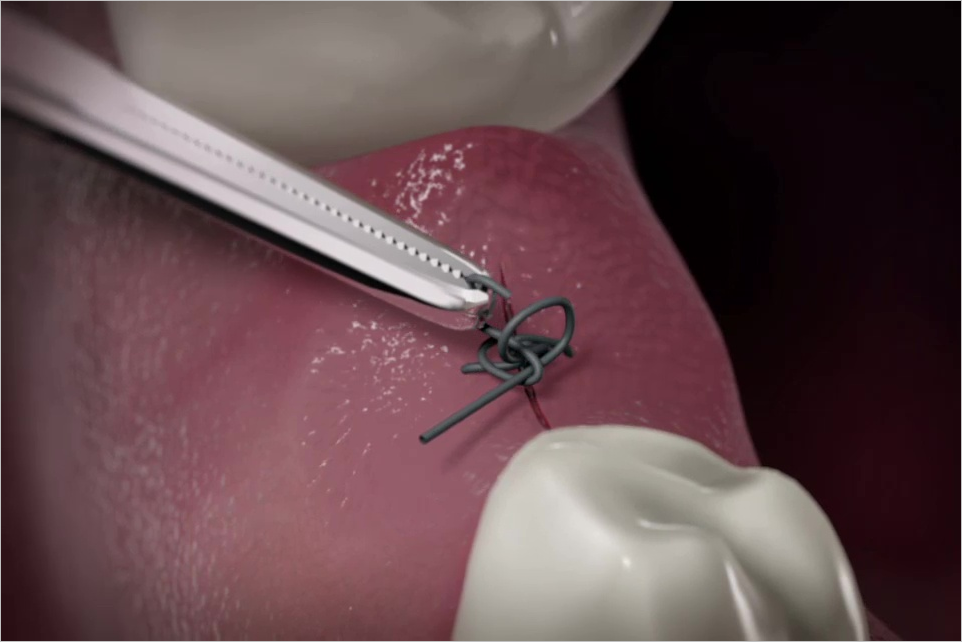
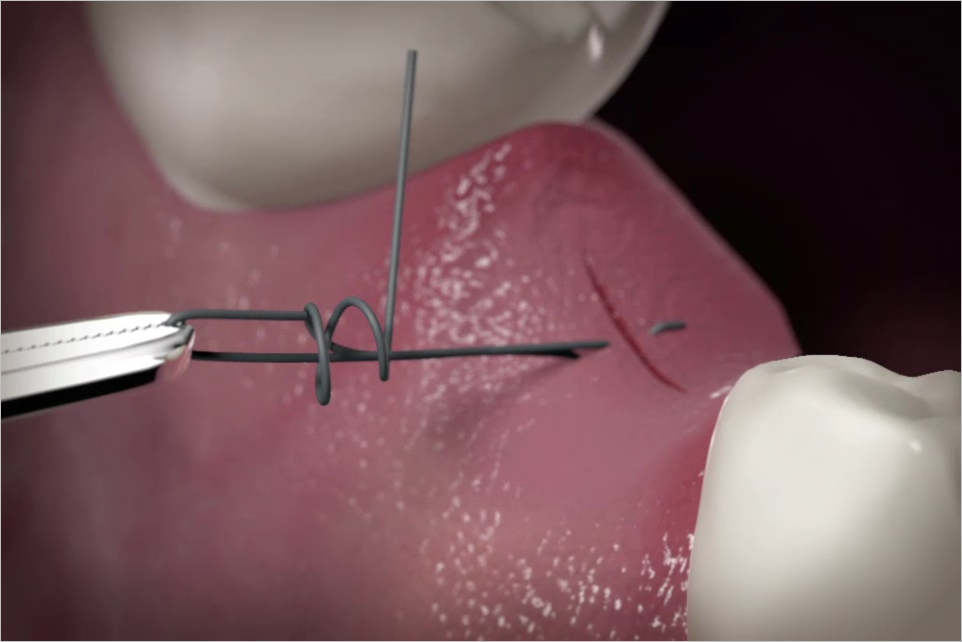
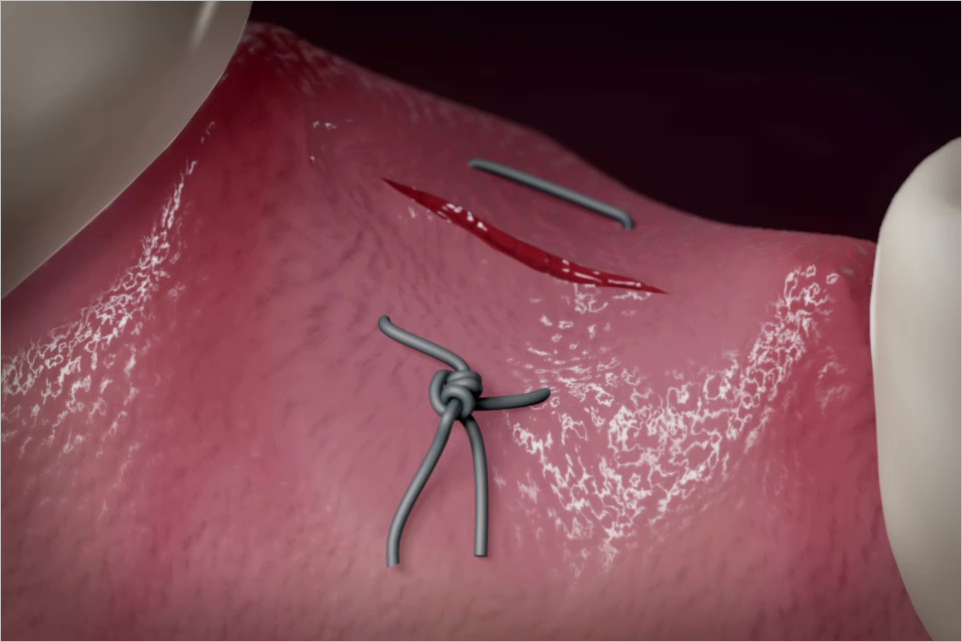
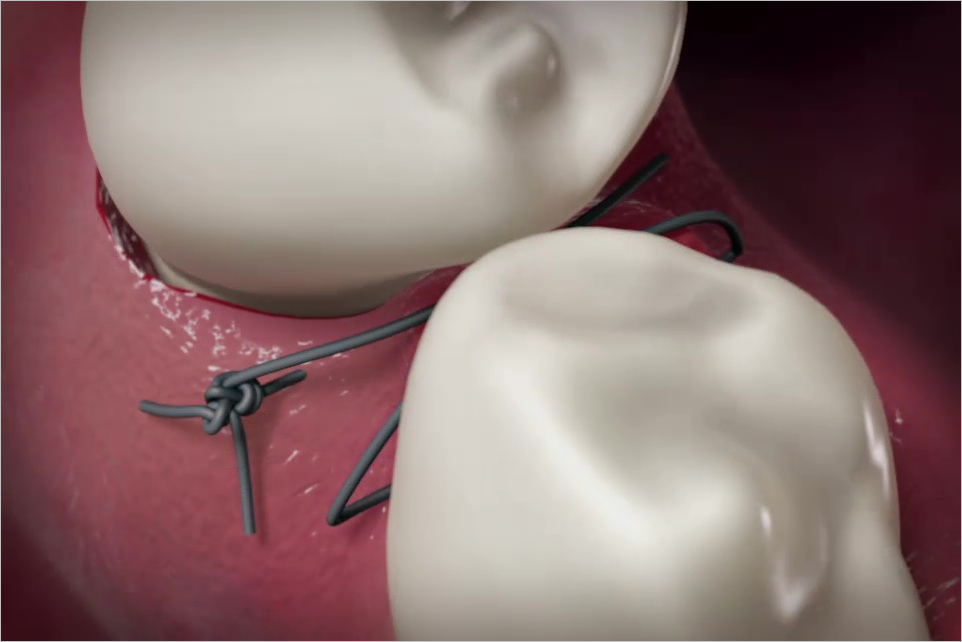
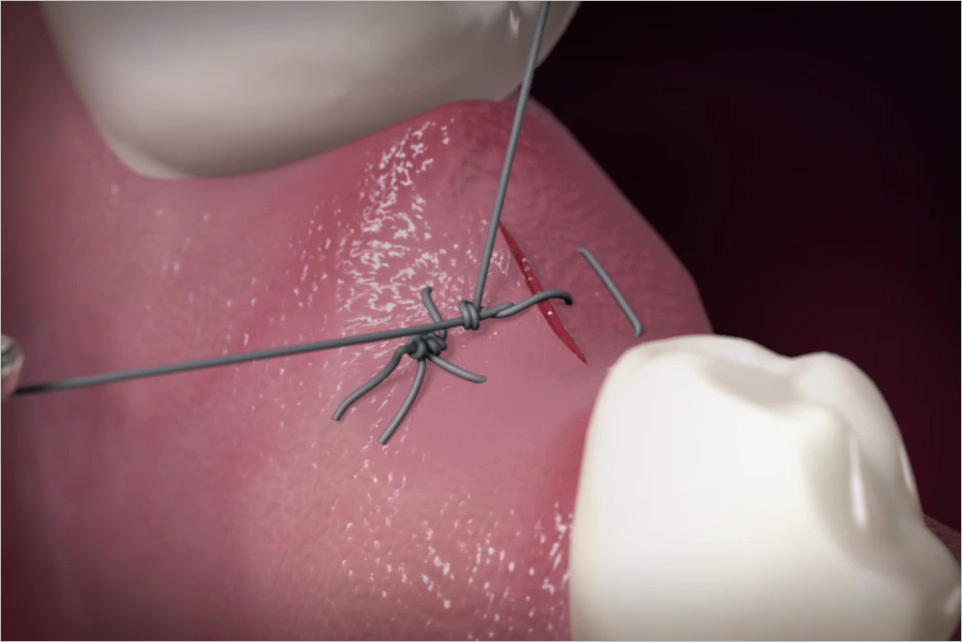
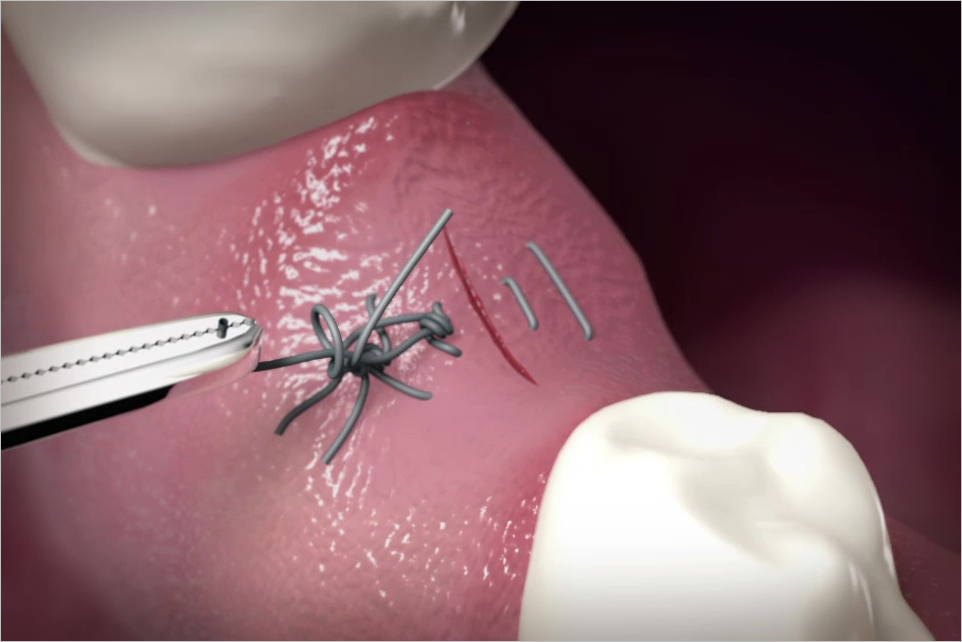
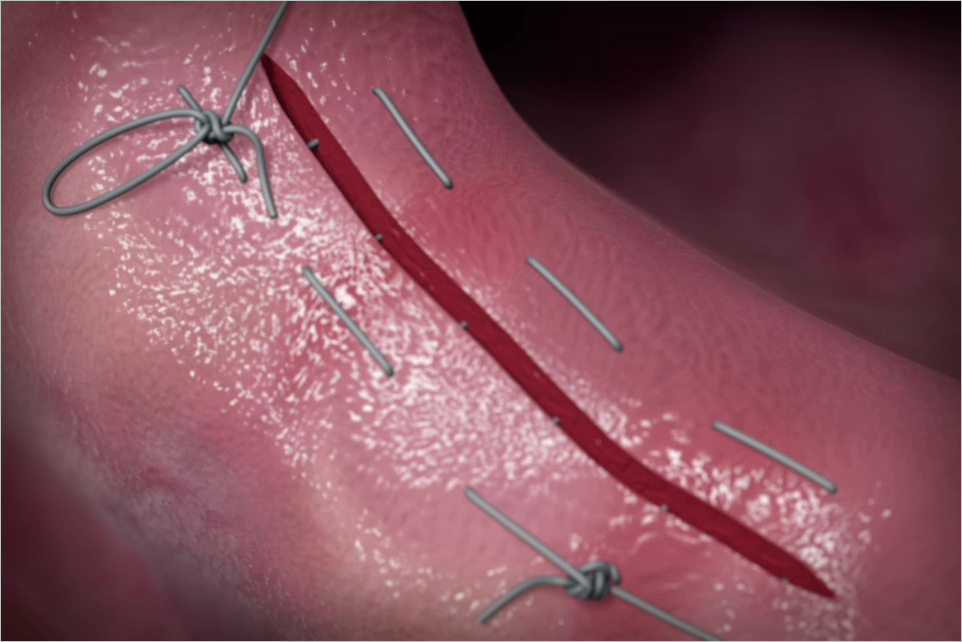
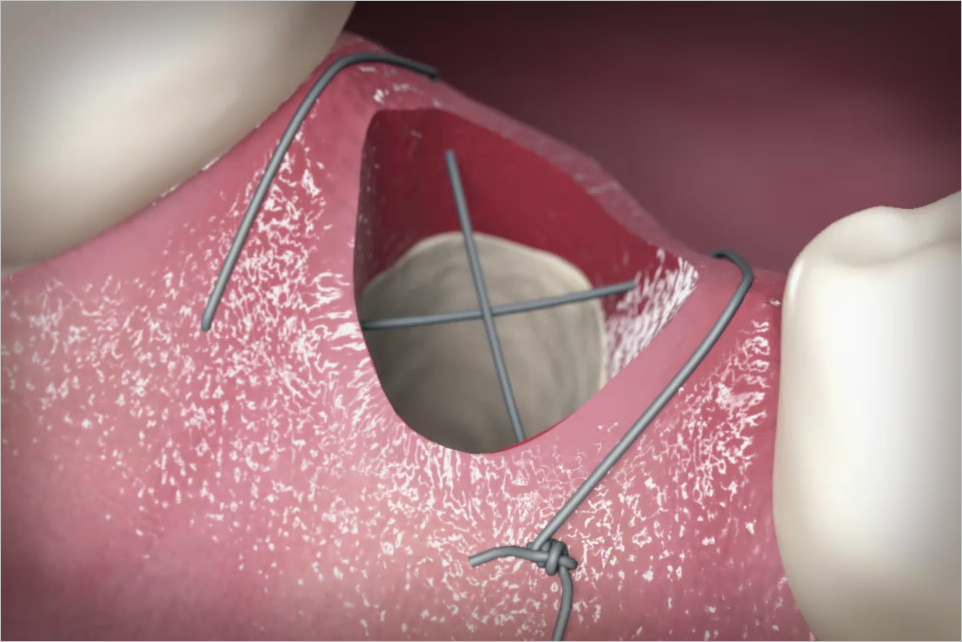
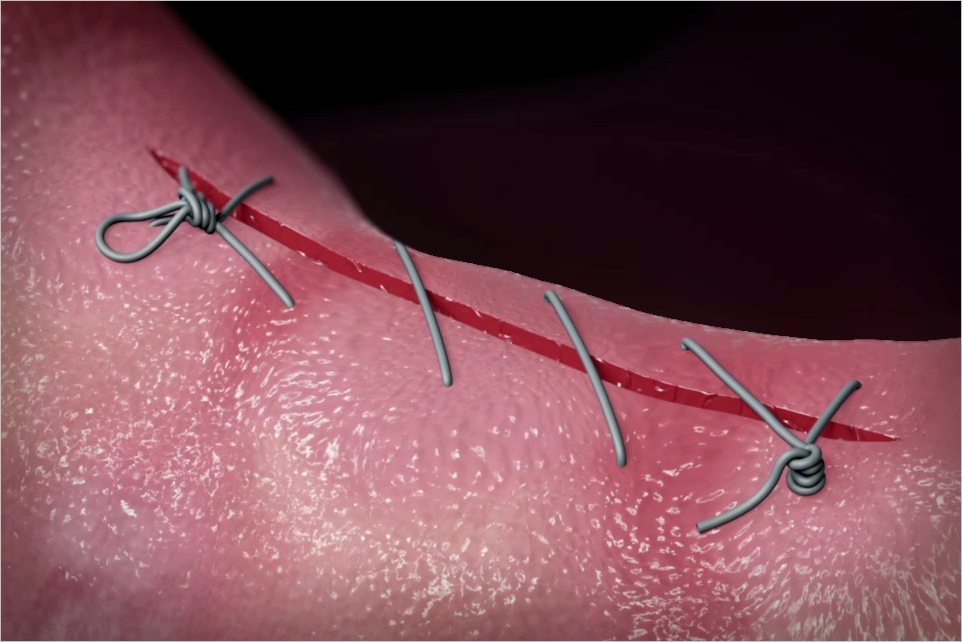
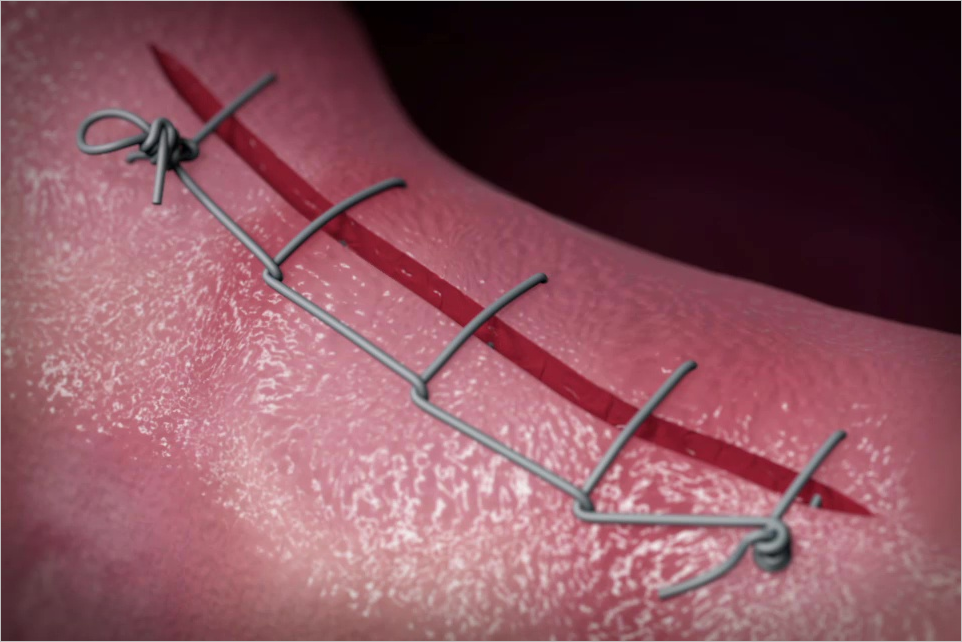
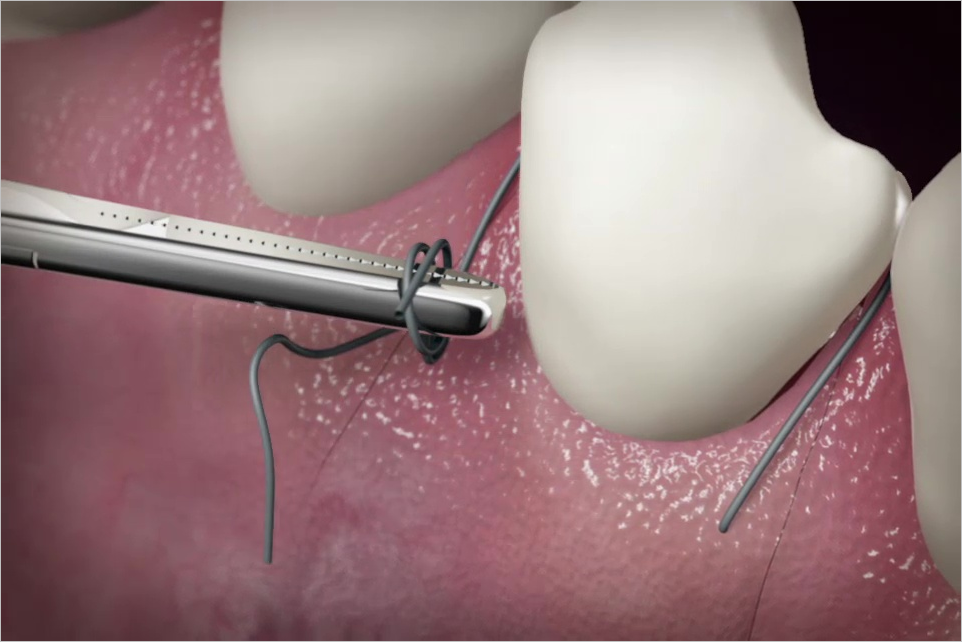
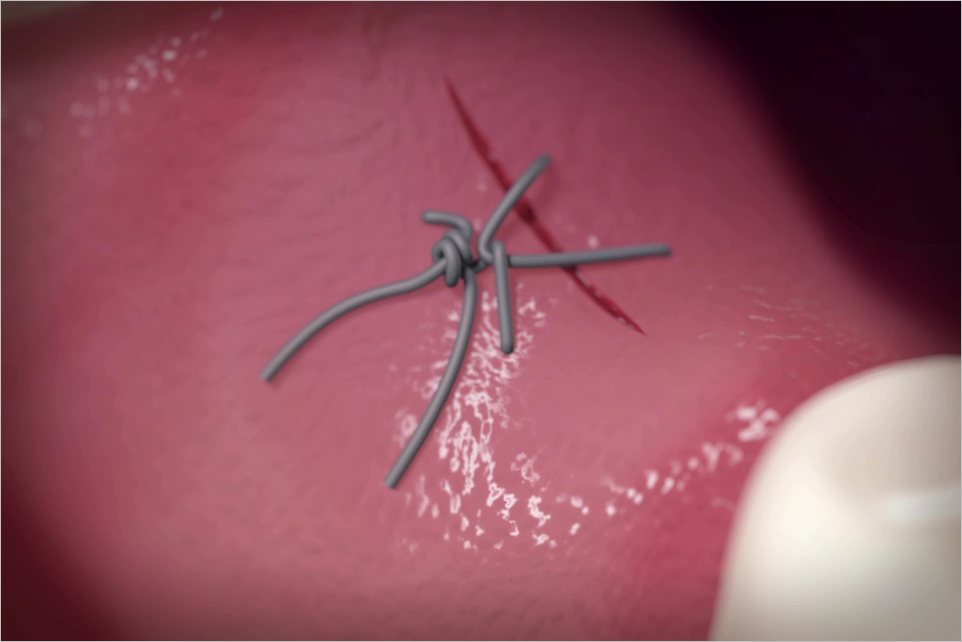
Interproximal attachment plays a crucial role in diagnosing periodontal conditions and predicting their prognosis due to its significant impact. The loss of interproximal attachment, often accompanied by papilla loss, can lead to phonetic, functional, and esthetic challenges. However, existing literature provides limited data on treatment outcomes for interdental papilla reconstruction and root coverage. This technical case report presents a novel surgical approach utilizing labial mucosal vertical incisions and palatal marginal vertical incisions to facilitate creation of a partial-full-thickness (PFT) tunnel. Then, connective tissue grafts (CTGs), stabilized by supra-crestal sling (SCS) sutures, are used to support and coronally advance the soft tissue overlying the graft to obtain root coverage and enhance papilla height and volume. This technique optimizes blood supply and maximizes wound stability, resulting in significant papilla augmentation and complete root coverage. It is suggested that PFT tunnel preparation via labial mucosal vertical incisions and palatal marginal vertical incisions, combined with CTG stabilization via the SCS suture, has the potential to treat gingival recessions with deficient papilla in the maxillary esthetic zone.
Palabras clave: connective tissue graft, papilla, periodontal surgery, root coverage
International Journal of Periodontics & Restorative Dentistry, 2/2025
DOI: 10.11607/prd.2025.2.c , ID de PubMed (PMID): 40048725Páginas 146-151, Idioma: InglésRasperini, Giulio / Avila-Ortiz, Gustavo / Pagni, Giorgio / Giannobile, William V.
This case series investigated the effect of a combination therapy utilizing connective tissue graft (CTG) in the treatment of periodontal regeneration of mandibular Class III/IV furcation involvement (FI). Six patients diagnosed with periodontitis stage III or IV (grade A to C), presenting with Class III or IV FI, were treated with fibroblast growth factor-2 and carbonate apatite in combination with CTG. The following clinical parameters were evaluated at baseline and after 6, 12, and 18 months: periodontal probing depth, clinical attachment level, furcation invasion, radiographic vertical defect depth, and gingival phenotype. Significant improvements in clinical parameters were observed in all treated FI sites. Four Class III defects and one Class IV defect obtained complete closure, and one Class IV defect was improved to Class I. This case series showed the potential of administering combination regenerative therapy for changing the prognosis of hopeless teeth with severe furcation defects.
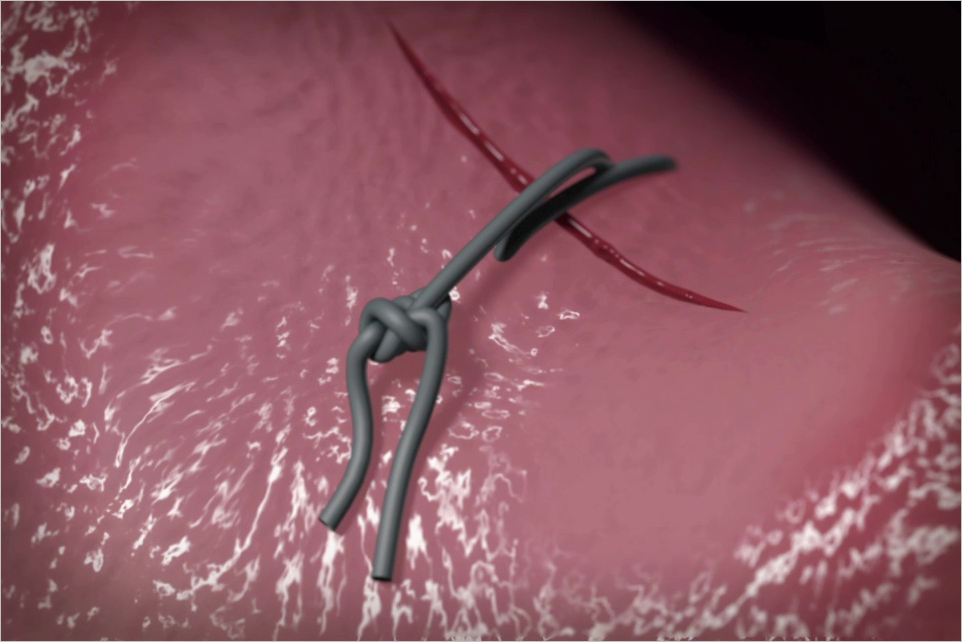
Surgical treatment of infrabony defects may result in gingival recession of the neighboring teeth. The aim of this clinical report is to describe a surgical technique to promote gingival margin stability in the treatment of infrabony defects at sites with a thin or medium gingival phenotype. A coronally advanced entire papilla preservation (CA-EPP) flap with a connective tissue graft (CTG) was executed in two different clinical cases. This technique substantially improved interproximal clinical attachment level and pocket closure, with no gingival recession. A CA-EPP flap using a CTG may promote gingival margin stability and can be recommended in regenerative periodontal procedures.
International Journal of Oral Implantology, 3/2023
ID de PubMed (PMID): 37767618Páginas 245-254, Idioma: InglésAlrmali, Abdusalam E / Saleh, Muhammad H A / Gnao, El-Hussein / Stuhr, Sandra / Rasperini, Giulio / Wang, Hom-Lay
Case presentation: Midfacial peri-implant soft tissue recession poses a significant challenge to achieving satisfactory aesthetic outcomes and requires a comprehensive, multidisciplinary approach. The present study describes two challenging cases in which implants were aesthetically compromised. A predictable technique was employed to manage these cases by using the implant itself as a tent to achieve 3D horizontal and vertical soft tissue building, which resulted in improved patient satisfaction. The first case involved a deep, severely buccally placed implant situated adjacent to compromised tooth structure. Horizontal and vertical soft tissue augmentation were carried out using a healing abutment to maintain the connective tissue coronal to the implant. The final fixed prosthesis was then delivered on top of the permanent submerged implant, with excellent soft tissue outcomes and a high level of patient satisfaction. The second case involved two compromised, deep, buccally placed implants that were managed by performing a permanent implant submergence technique on the maxillary left central incisor implant and augmenting the soft tissue vertically and horizontally. The final fixed prosthesis was delivered between the maxillary left lateral incisor implant and the previously prepared maxillary right central incisor, resulting in an acceptable aesthetic outcome. The technique presented managed the peri-implant soft tissue dehiscence effectively and restored the previously deficient peri-implant papillae.
Conclusions: The key to treating challenging aesthetic complications encountered with implants is presurgical prosthetic preparation followed by use of a comprehensive surgical technique to optimise soft tissue thickness and height and address compromised aesthetics in a single surgical step. Use of a permanent implant submergence technique with remediation of associated defects may be a viable clinical approach that is not often explored for these types of defects.
Palabras clave: aesthetics, connective tissue, dental implants, single-tooth
The authors report no conflicts of interest relating to this study.
The aim of the present study was to evaluate, clinically and via CBCT, the long-term efficacy of a bioresorbable polylactic acid membrane combined with deproteinized bovine bone graft (DBBM) and compare it to enamel matrix derivative (EMD) combined with DBBM graft in the treatment of class II furcation defects. Sites were randomly assigned to the test group (Guidor Matrix Barrier + Bio-Oss) or the control group (Emdogain + Bio-Oss). Probing pocket depth (PPD), clinical attachment level (CAL), gingival recession (REC), and keratinized tissue (KT) width were assessed at 12 and 24 months, and radiographic bone gain was investigated at 24 months via CBCT. Both groups showed a significant radiographic bone fill and clinical gain. The combination of Emdogain + Bio-Oss showed better clinical outcomes and less complications, though this difference was not statistically significant.
The present study introduces a novel "anatomic recession ratio" (ARR) and evaluates the clinical outcomes of using a tunnel technique (TUN) with a connective tissue graft (CTG) for root coverage (RC). Sixteen systemically healthy patients contributing a total of 33 recession types 1 and 2 were treated with TUN + CTG. The predictive value of a panel of baseline clinical parameters (ARR) on RC was evaluated 12 months postoperatively. At 12 months, mean recession depth decreased from 2.74 ± 0.22 mm to 0.46 ± 0.13 mm (P < .0001); 19 sites (58%) showed complete RC, and the mean RC rate was 88.85% ± 2.73%. The mean ARR value was 0.74 ± 0.3, revealing a positive correlation with RC (r2: 0.73, P < .0001). The 12-month esthetic evaluation resulted in a score of 8.52 ± 1.75 using the root coverage esthetic score. TUN + CTG is effective in reducing recession depth and obtaining good esthetic outcomes. Within the limits of the present study, it may be suggested that ARR has potential as an analytical baseline parameter for RC outcomes with TUN + CTG.
The aim of the present study was to generate an international and multidisciplinary consensus on the clinical management of implant protrusion into the maxillary sinuses and nasal fossae. A total of 31 experts participated, 23 of whom were experts in implantology (periodontologists, maxillofacial surgeons and implantologists), 6 were otolaryngologists and 2 were radiologists. All the participants were informed of the current scientific knowledge on the topic based on a systematic search of the literature. A list of statements was created and divided into three surveys: one for all participants, one for implant providers and radiologists and one for otolaryngologists and radiologists. A consensus was reached on 15 out of 17 statements. According to the participants, osseointegrated implants protruding radiographically into the maxillary sinus or nasal fossae require as much monitoring and maintenance as implants fully covered by bone. In the event of symptoms of sinusitis, collaboration between implant providers and otolaryngologists is required. Implant removal should be considered only after pharmacological and surgical management of sinusitis have failed.
Palabras clave: consensus, dental implants, maxillary sinus, nasal fossae
Conflict-of-interest statement: The authors declare there are no conflicts of interest relating to this study.
Kariesläsionen mit tiefen Rändern sind in der zahnärztlichen Praxis erhebliche Herausforderungen. Folgende Schlüsselaspekte dieses Problems werden im vorliegenden Beitrag diskutiert: Wie ist unter restaurativem Gesichtspunkt mit einem tiefen Kavitätenrand umzugehen? Wann und wie sollte chirurgisch interveniert werden? Welcher ist der beste Zeitpunkt für die definitive restaurative Versorgung nach einer chirurgischen Intervention? Die mittlerweile verfügbaren Restaurationsmaterialien und Adhäsivtechniken ermöglichen minimalinvasive Behandlungsansätze und damit einen umfangreichen Substanzerhalt und helfen dabei, unerwünschte Reaktionen der parodontalen Gewebe zu vermeiden. Je nach klinischer Ausgangslage kommen bei subgingivalen Kavitätenrändern drei Behandlungsoptionen in Betracht. Liegt der Rand maximal 1,5 mm unter dem Gingivarand, ist eine Anhebung des Kavitätenrands unter Kofferdam möglich, was eine optimale Restauration und Weichgewebeintegration erlaubt. Liegt der Kavitätenrand mehr als 1,5 mm unter dem Gingivarand, ist vor der Restauration eine chirurgische Intervention erforderlich. Liegt der Rand noch mindestens 2 mm über dem Knochen, wird ein ästhetisches suprakrestales Gewebemanagement (Supracrestal Tissue Esthetic Management, STEM) durchgeführt. Das heißt, es genügt eine Osteoplastik, um das suprakrestale Attachment neu zu etablieren und die restaurative Behandlung durchführen zu können. Eine Ostektomie ist nicht nötig. Liegt der Kavitätenrand weniger als 2 mm koronal zum Knochenkamm, ist eine Kronenverlängerung mit einer minimalen Ostektomie und anschließenden Osteoplastik indiziert.
Carious lesions with deep margins represent a challenge in daily clinical practice. The following key points are discussed in this article: how to manage a deep margin from a restorative point of view; when and how to perform a surgical procedure; and when it is favorable to carry out definitive restoration work after surgery. The restorative materials and adhesive procedures available today allow minimally invasive techniques to be used on dental tissue with a high preservation of tooth structure. These materials and techniques help to avoid adverse periodontal tissue reactions. Depending on the clinical situation, three treatment options are available when dealing with a subgingival margin. If the depth of the cavity margin is at a maximum distance of 1.5 mm below the gingival margin, isolation with rubber dam allows the performance of interproximal margin relocation, thereby facilitating optimal restoration and periodontal tissue integration. If the margin is located deeper than 1.5 mm below the gingival margin, surgery is necessary before any restorative work can take place. When the margin is within 2 mm above the bone crest, a supracrestal tissue esthetic management (STEM) procedure is undertaken, which means that no ostectomy is required and only osteoplasty is necessary to reshape the preexisting supracrestal attachment, thereby allowing the restorative work to proceed. When the margin is less than 2 mm above the bone crest, crown lengthening with minimal ostectomy and subsequent osteoplasty becomes necessary.